Thyroid US Reader
An AI system that processes thyroid ultrasound studies and generates ACR TI-RADS compliant structured radiology reports. Addresses the most cognitively demanding, time-inefficient task in daily radiology practice.
Research System - Not FDA Cleared. This system is used solely for internal research, development, and technical validation purposes by the founding physician-engineer. It does not constitute a medical device, clinical decision support system, or diagnostic tool. All AI outputs require review and authorization by a licensed physician before any clinical application. VoxelMD is not intended to replace physician judgment. No patient data is processed or stored through this system.
The Clinical Problem
Thyroid ultrasound reporting is one of the highest-volume, lowest-margin, most cognitively demanding tasks in outpatient radiology - and it remains entirely manual.
600K-1M
Thyroid US Studies / Year (US)
CPT 76536 is one of the most frequently ordered outpatient radiology exams, driven by the 19-68% nodule prevalence in adults undergoing cervical imaging.
5 categories
Per Nodule, Per Patient - Manually
ACR TI-RADS requires structured evaluation of composition, echogenicity, shape, margin, and echogenic foci for every nodule - documented in a structured dictation.
$300M+
US Addressable Market
Low-reimbursement, high time-cost studies that reduce radiologist throughput. A shortage of 42,000 radiologists projected by 2050 makes automation a structural necessity.
How It Works
An AI system that accurately produces structured reports from complex multi-image thyroid ultrasound studies — solving the challenge that makes thyroid US reporting so time-consuming.
Thyroid ultrasound study - bilateral anatomy, two planes, burned-in annotations
Every score grounded in image evidence
ACR TI-RADS compliant, mapped to your EHR schema
Illustrative example output
Study Ingestion
A thyroid ultrasound study arrives - typically 30 to 80 DICOM images spanning multiple nodules, bilateral anatomy, and two imaging planes. No metadata maps images to nodules. The only ground truth is the ultrasound machine's text overlay burned into each image's pixel space.
Image Classification - Spatial Mapping
The system intelligently organizes each image by anatomical side, imaging plane, caliper presence, and nodule identity — attributing every image to the correct finding before any diagnostic reasoning begins.
Structured Reporting - ACR TI-RADS Evaluation
The system evaluates all 5 TI-RADS categories per nodule following ACR TI-RADS scoring standards. Built-in hallucination prevention ensures every feature score is grounded in actual image evidence.
Structured Report Generation
The system generates a complete field-level structured report: per-nodule TI-RADS scoring, nodule dimensions, laterality, composition, echogenicity, margin classification, echogenic foci, and ACR-compliant follow-up recommendations. Output conforms to EHR data schemas for direct ingestion - not just narrative text.
Continuous Improvement Loop
When a radiologist reviews and corrects a generated report, the system learns from the correction and adapts to your reading preferences. Accuracy compounds with every study — the system gets better the more your practice uses it.
System in Action
A screen recording demonstrating the VoxelVision thyroid ultrasound reporting pipeline.
Internal research demonstration. No patient data. For technical evaluation purposes only.
Structured Report Output
Screenshots of the VoxelVision interface generating ACR TI-RADS compliant structured reports from live DICOM studies. Each field is AI-populated - composition, echogenicity, margin, echogenic foci, TI-RADS score, and EHR-ready follow-up recommendation.
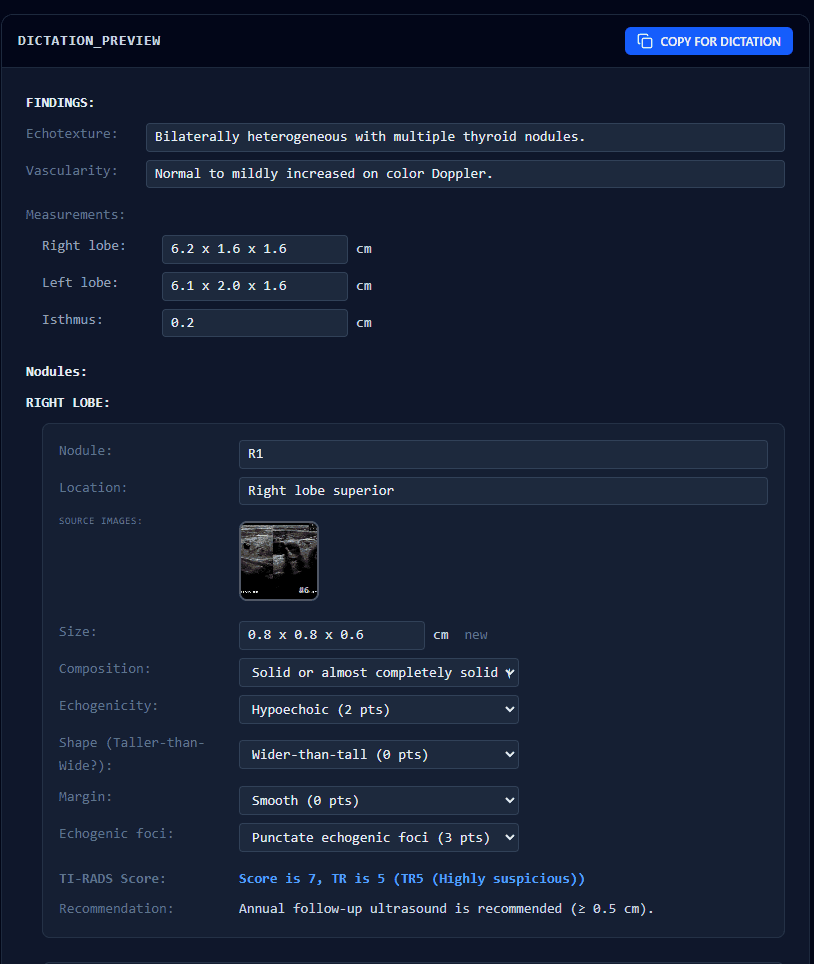
Nodule R1 (Right Lobe Superior) - AI assigned TI-RADS Score 7, TR5 (Highly Suspicious) based on hypoechoic composition, punctate echogenic foci, and caliper-confirmed 0.8 × 0.8 × 0.6 cm dimensions. Source DICOM frame is thumbnailed directly in the report.
EHR-compatible field-level output: bilateral measurements, vascularity, echotexture, per-nodule TI-RADS scoring, and ACR-compliant follow-up recommendation - ready for direct PACS / EHR ingestion.
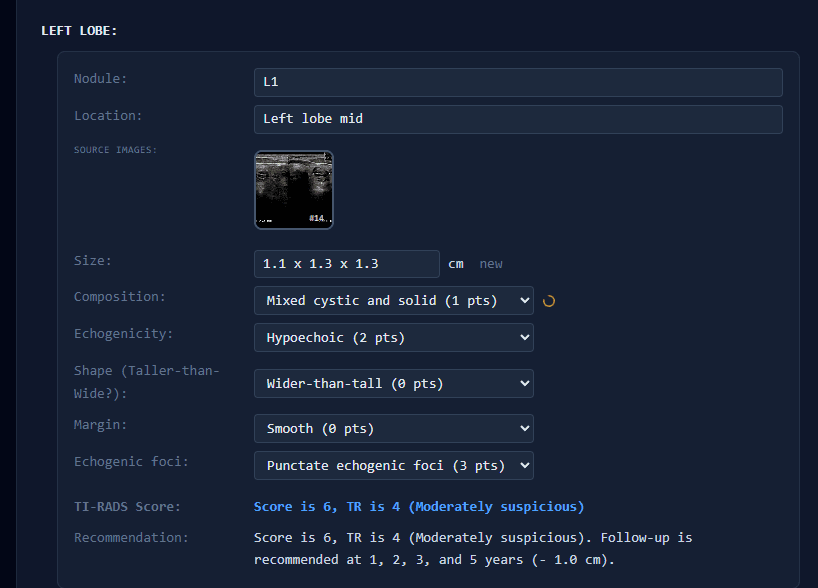
Nodule L1 (Left Lobe Mid) - AI scored TI-RADS 6, TR4 (Moderately Suspicious): mixed cystic and solid composition, hypoechoic, punctate echogenic foci. Follow-up recommendation generated at 1, 2, 3, and 5 years per ACR guidelines.
Multi-nodule studies are handled independently - each nodule receives its own isolated image set, scoring chain, and follow-up recommendation, preventing cross-contamination of findings between anatomical sites.
6 nodules identified across bilateral anatomy, 46 images classified - the system resolved spatial attribution for every image before generating a single field of the report. All output is structured JSON mapped to EHR field schemas, not narrative prose.
Four Core Challenges We Solved
Each challenge is specific to thyroid ultrasound reporting. Each has a defined success metric.
Spatial Mapping Across Multi-Image Studies
Challenge
30-80 images across multiple nodules and bilateral anatomy with no metadata linking images to nodules. A generalist VLM cross-contaminates findings between nodules.
Approach
Proprietary spatial mapping technology organizes every image by anatomy, imaging plane, and nodule identity before any diagnostic reasoning begins.
Success Metric
≥ 95% image classification accuracy across 500 heterogeneous studies vs. radiologist-annotated ground truth
TI-RADS Hallucination Prevention
Challenge
Evaluating echogenicity or composition in noisy ultrasound images - a VLM is prone to generating plausible but unsupported feature scores without visual evidence.
Approach
Built-in hallucination prevention technology ensures every feature score is grounded in actual image evidence.
Success Metric
< 2% feature-level hallucination rate across 200 blinded cases, validated by subspecialty radiologist review
EHR-Compliant Structured Output
Challenge
Text that sounds like a radiology report is insufficient. Output must conform to field-level EHR data schemas - TI-RADS score, nodule size, laterality, follow-up encoding - for direct ingestion.
Approach
Constrained output schema enforcement at inference time. Output is field-mapped to EHR schemas, not narrative text. PACS-compatible delivery.
Success Metric
≥ 90% categorical agreement on TI-RADS category and follow-up across 1,000 consecutive de-identified cases; ≥ 85% clinically usable by a panel of 3 subspecialty radiologists
Automated Clinical Rule Extraction
Challenge
The self-improvement loop depends on correctly interpreting what a radiologist correction means clinically. Incorrectly generalizing a correction can degrade performance.
Approach
Proprietary learning technology validates every correction before incorporation, ensuring accuracy compounds over time.
Success Metric
Instruction updates that improve concordance on a held-out validation set in ≥ 80% of feedback cases
Adapts to Your Reading Style
The more your radiologists use VoxelVision, the more accurately it reflects their preferences, terminology, and clinical standards. A system that gets better every day.
AI drafts the report
structured, signable
Radiologist reviews & signs
full control, always
Corrections are captured
terminology, style, thresholds
The next report is better
no retraining cycle
Step 04 feeds step 01 - accuracy compounds at your institution
Institution-Specific
Adapts to each practice's preferences, terminology, and clinical standards over time.
Instant Learning
Every correction is immediately incorporated — no waiting for model retraining or software updates.
Compounding Accuracy
The longer your practice uses VoxelVision, the more accurate and tailored it becomes.
Cloud Infrastructure
The system runs on Google Cloud for all inference. Medical images are de-identified before any cloud transmission. All proprietary components remain under VoxelMD control.
Phase II Requires
- Advanced model training infrastructure
- Cloud-based fine-tuning capabilities
- High-performance GPU compute for 3D imaging
- Secure storage for training data and models
Market Opportunity
600K-1M
Studies/Year (US)
CPT 76536 thyroid ultrasound
$300M+
Addressable Market
US thyroid US AI reporting
80%
Dictation Time Reduction
Internal estimation
A system that keeps getting better: Each radiologist correction makes the system more accurate for that practice. The longer a group uses VoxelMD, the more accurate and tailored it becomes - a system that keeps getting better.
VoxelMD products are in active research and development. Nothing on this website constitutes a cleared or approved medical device, clinical decision support system, or FDA-regulated software as a medical device (SaMD). No VoxelMD system is cleared or approved by the FDA or any regulatory body for clinical use. All AI outputs are for research and development purposes only and require review and authorization by a licensed physician before any clinical application. Performance metrics referenced are based on internal technical testing and have not been independently validated. Silicon Health Solutions LLC (d/b/a VoxelMD) is a California-registered company.
Explore the Full System
Deployment options, expanding coverage, and product roadmap.